BREAST RECONSTRUCTION
AUTOLOGOUS RECONSTRUCTION
The decision which method should be used in the reconstruction should be made with great care and above all, without time pressure. You should obtain comprehensive information about the different methods and surgical techniques beforehand. Do not hesitate to get an independent second opinion from a plastic surgeon with ample experience in the field of breast reconstruction before making your decision.
A good reconstructive result can improve your quality of life significantly and restore your physical integrity. Autologous reconstruction, to which experts refer as flap technique, is conducted using exclusively microsurgical techniques in modern centers for breast surgery. Skin and fatty tissues are extracted from the selected part of the body (abdomen, buttocks or thighs) without damaging the muscular tissue underneath.
The tissue is then connected to the vessels on the chest wall and shaped into a new breast. The most intricate part of the surgery is the opening and the connection of the blood vessels of the extracted tissue flap to the vessels of the chest wall. In this procedure, veins and arteries with a diameter of less than 1mm are connected with approx. twelve stitches under the microscope to ensure that the inserted tissues in the breast are supplied with blood sufficiently.
THE MOST COMMON SURGICAL METHODS IN AUTOLOGOUS RECONSTRUCTION ARE:
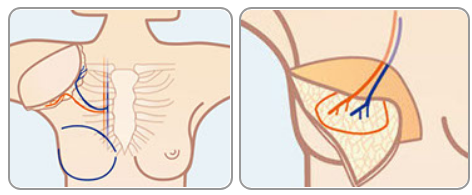
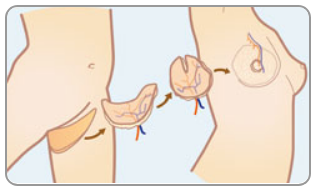
1. DIEP flap
using tissue from the lower abdomen
The DIEP flap method entails the extraction of an oval flap of tissue from the abdomen underneath the naval to be used as donor material for the new breast. The rectus muscle remains intact which is a decisive advantage with respect to recovery time in comparison to other methods. The lower abdomen is closed like an aesthetic abdominoplasty – a side effect of this method that is appreciated by many patients. The abdominal fat flap can be used to reconstruct one or two breasts.
2. S-GAP of I-GAP flaps
using tissue from the buttocks
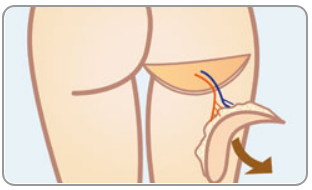
If the abdomen does not have enough fatty tissue that can be extracted, or if the tissue has been damaged in a previous operation, the donor tissue can be extracted from the buttocks. Using this method it is also possible to reconstruct one or both breasts.
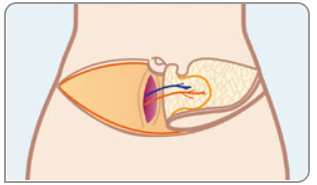
3. TMG flap
using tissue from the inner side of the upper limb
Alternatively, the donor tissue can be extracted from the inner side of the thigh underneath the gluteal fold. With this method, the scar is located in the crotch and is particularly unobtrusive. A positive side effect of this method is the fact, that the skin of the thigh is tightened at the same time.
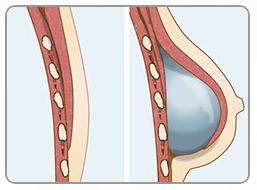
RECONSTRUCTION WITH SILICONE IMPLANTS
Breast reconstruction with silicone implants in connection with a skin sparing mastectomy in one procedure (primary reconstruction) is frequently the first choice in reconstructive methods for gynecological clinics. However, it is hard for many women to imagine living with a foreign body in their chest permanently. In addition, problems with the implants may occur later in connection with radiation treatment. In that case, secondary or an autologous reconstruction of the breast at a later point in time may be advisable.
Immediate breast reconstruction using silicone implants is one of the easiest surgical reconstruction methods. The most important disadvantage of this method is that the human body does recognize the implant as a foreign body in the long run and tries to encapsulate it by creating additional connective tissue. The surface of the latest generation of implants counteracts this process; the development of anatomically shaped implants has led to a significant improvement of reconstruction results.
In order to create a natural breast it is necessary to have a sufficient amount of skin. If there is not enough skin, the skin has to be overstretched for a certain period of time. A temporary skin expander is used for this purpose. Afterwards, the skin has to rest for two to three months.
If possible, the implant is placed behind the detached pectoral muscle. In order to achieve a sufficient coverage of the implant by soft tissue, an additional mesh may be placed around the pectoral muscle and the implant.